Happy March! Today, I spent the lovely day inside the lab, reading. The reason I have to read different kinds of articles is to learn different TMS techniques. So I read an article for our Journal Club titled "Low-Frequency Repetitive TMS Plus Anodal Transcranial DCS Prevents Transient Decline in Bimanual Movement Induced by Contralesional Inhibitory rTMS After Stroke." So what does that mean? Let's start with a little review.
Last post, I talked about modes of TMS, and rTMS was one of them. rTMS is not "dark" as suggested in my title. In fact, it is used for therapeutic applications, such as after strokes. In strokes, parts of the brain are affected and disabled. For the subjects in this article, one side of the brain was affected, and when one side of the brain is disabled, the unaffected half of the brain works harder to compensate for the missing parts in the other side of the brain, basically working for those disabled areas. The brain's ability to adapt such as in cases like these is called
neuroplasticity. So when stimulating the unaffected side with rTMS, the stimulation is seen also in the affected half of the brain. The reason they used the rTMS on the unaffected side was to increase the neuroplasticity, so this is a treatment for stroke patients.
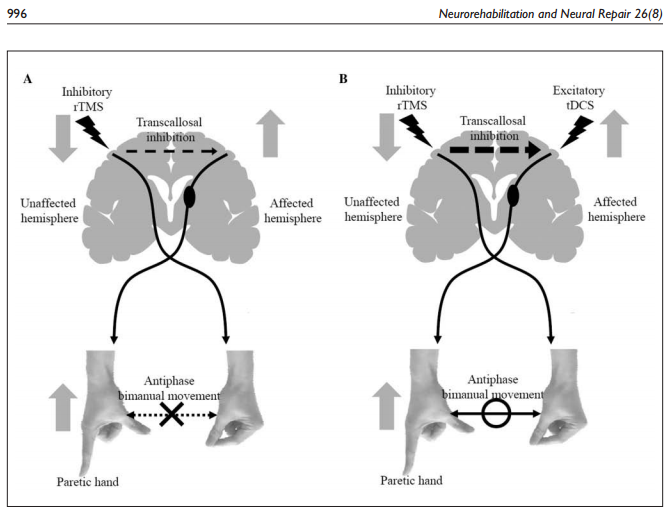
But rTMS has a dark side. It has a negative effect on bimanual movement, decreasing the ability for a person to move both hands. To negate this effect, transcranial direct current stimulation (tDCS) was used. tDCS is not a type of TMS. In fact, tDCS is weaker than TMS and is less prone to cause seizures (to learn more about tDCS, click
here). The tDCS was able to counteract the bad side of rTMS, allowing the subjects the ability of bimanual movement.
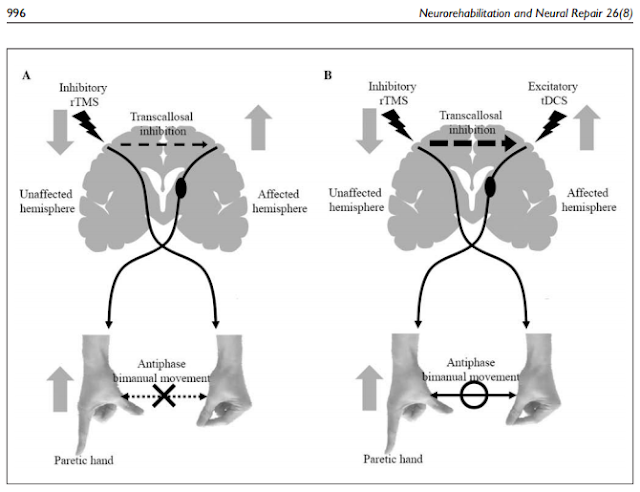 |
| This picture illustrates the effect of the tDCS against rTMS, as I had stated above. (Picture taken from article) |
References:
- Takeuchi, N.; Tada, T.; Matsuo, Y.; Ikoma, K.Low-frequency repetitive TMS plus anodal transcranial DCS prevents transient decline in bimanual movement induced by contralesional inhibitory rTMS after stroke. Neurorehabil Neural Repair 2012, 26: 988-999.